
UNMC Project — Digital Health Platform for Sickle Cell & Malaria Screening
Led business analysis and product coordination for the SMART initiative with the University of Nebraska Medical Center, delivering a digital health platform for sickle cell and malaria screening in low-resource settings. Translated complex clinical workflows into scalable Android/Web applications integrated with portable diagnostic hardware, helping achieve 97.2% diagnostic accuracy and accelerating early intervention for at-risk children.
Role
Business Analyst
Timeline
In Development
Team
University of Nebraska Medical Center (UNMC)
1. Executive Summary
The SMART (Sickle and Malaria Accurate Remote Testing) initiative, developed with the University of Nebraska Medical Center, delivered a digital health platform for sickle cell and malaria screening in low-resource settings across Nigeria. As a Business Analyst, I led clinical workflow analysis, requirements strategy, and cross-functional coordination for an Android/Web ecosystem integrated with portable diagnostic hardware. The platform achieved 97.2% diagnostic accuracy and enabled significantly earlier intervention for infants at risk of sickle cell disease.

Healthcare worker using the app to support early sickle cell screening in low-resource clinical environments.
2. My Role & Ownership
As a Business Analyst, I supported clinical workflow analysis, requirements gathering, backlog documentation, and cross-functional coordination between clinical stakeholders and engineering teams. I helped translate complex medical and operational workflows into structured software requirements for the Android/Web platform, while contributing to workflow design, validation logic, and implementation planning throughout the project lifecycle.
3. Context & Problem
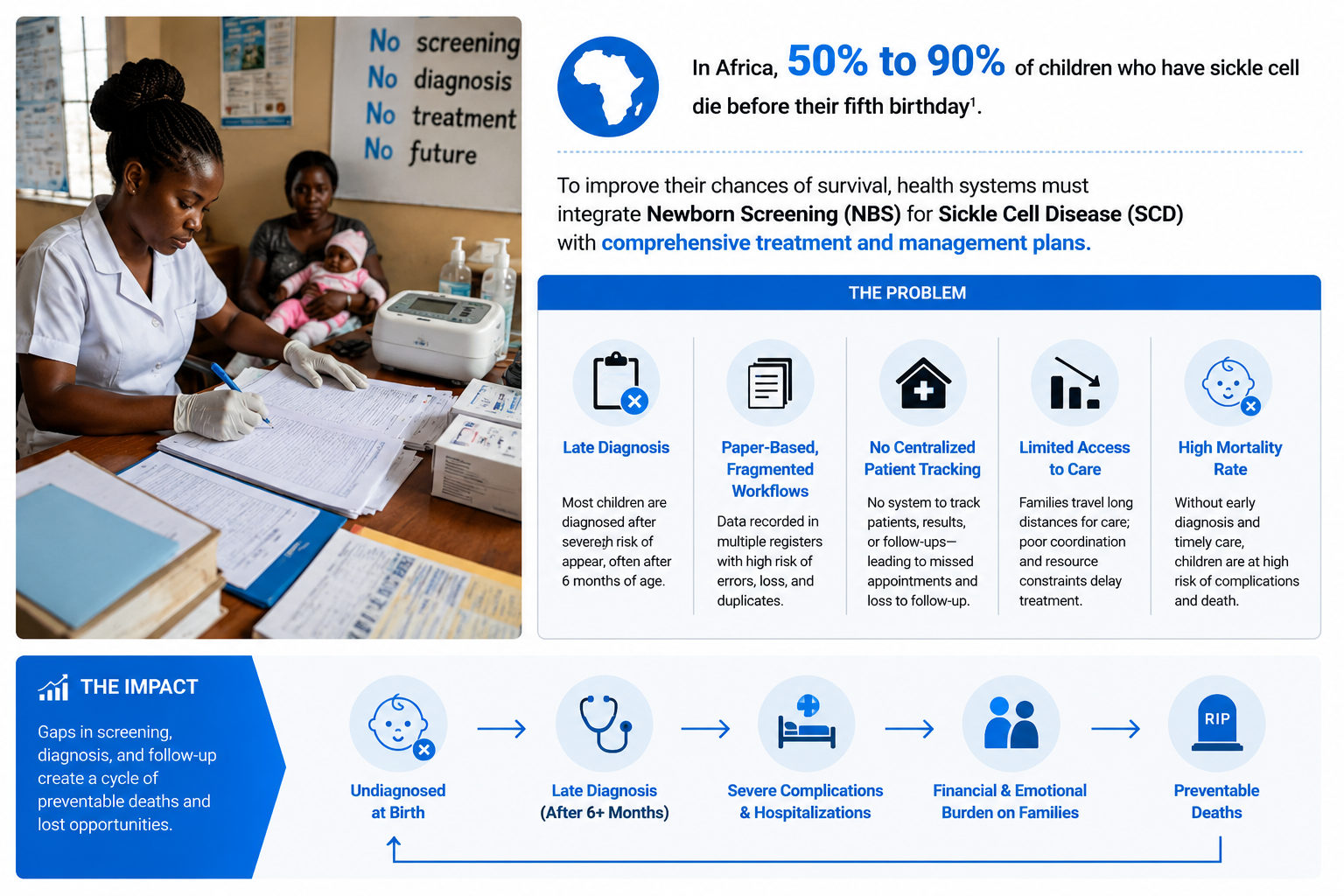
Sickle cell disease remains one of the leading causes of preventable child mortality in sub-Saharan Africa, with nearly 250,000 babies born annually with the condition. In many low-resource regions, infants are not diagnosed early enough to receive timely treatment, contributing to mortality rates as high as 50–90% before age five1. Existing diagnostic workflows were fragmented, paper-driven, and difficult to scale across remote environments with limited electricity and inconsistent connectivity. Healthcare workers also lacked centralized systems to longitudinally track patients, laboratory results, and follow-up care throughout the diagnostic journey.
4. Key Insight
The core insight was that diagnostic technology alone could not meaningfully improve patient outcomes without an integrated digital workflow system. While the Gazelle Hb Variant point-of-care diagnostic device enabled rapid screening in the field, healthcare workers still lacked reliable tools for patient registration, continuous patient tracking, laboratory workflows, and follow-up care. By combining point-of-care diagnostics with centralized digital records and structured clinical workflows, the platform transformed screening from a one-time diagnostic event into a continuous patient management process that supported earlier intervention and improved care coordination.
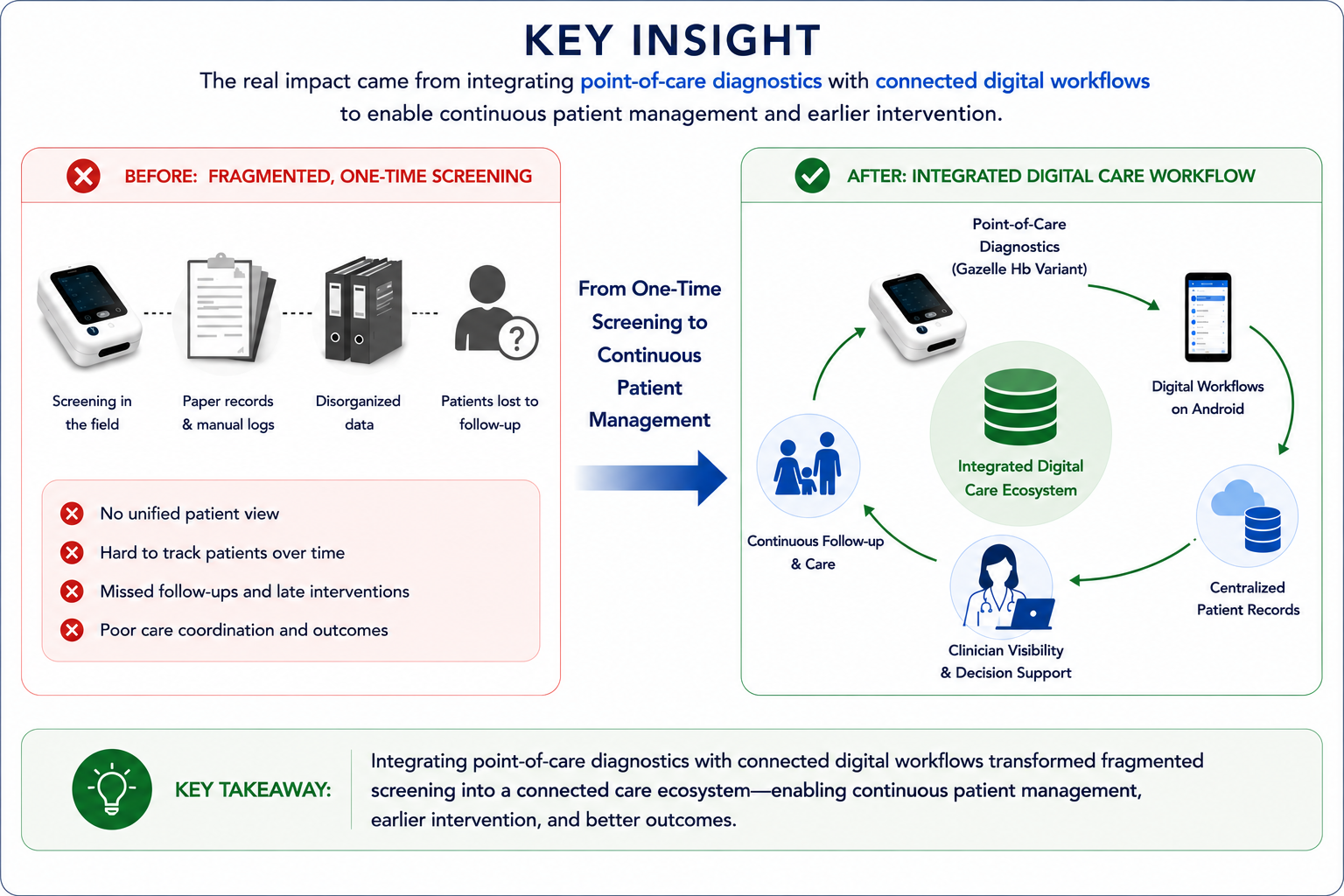
Integrating point-of-care diagnostics with connected digital workflows transformed fragmented screening processes into a continuous patient management ecosystem supporting earlier intervention, coordinated follow-up care, and improved clinical outcomes.
5. Vision & Strategy
The vision for the UNMC Project was to establish a scalable digital health ecosystem capable of supporting early sickle cell diagnosis, continuous patient management, and centralized clinical oversight in low-resource settings. Rather than treating screening as a standalone diagnostic event, the platform was designed to connect point-of-care diagnostics, mobile clinical workflows, centralized patient records, and administrative oversight into a unified care coordination system.
The strategy focused on building a phased, operationally practical platform that could support both frontline healthcare workers and researchers simultaneously. Android applications enabled field teams to capture patient registration, clinical evaluations, biometrics, and laboratory workflows directly at the point of care, while the web application provided centralized administration, laboratory monitoring, biometric matching, role-based access management, and research oversight. This hub-and-spoke architecture created a scalable foundation for continuous patient tracking, earlier intervention, and data-driven healthcare decision-making across distributed clinical environments.
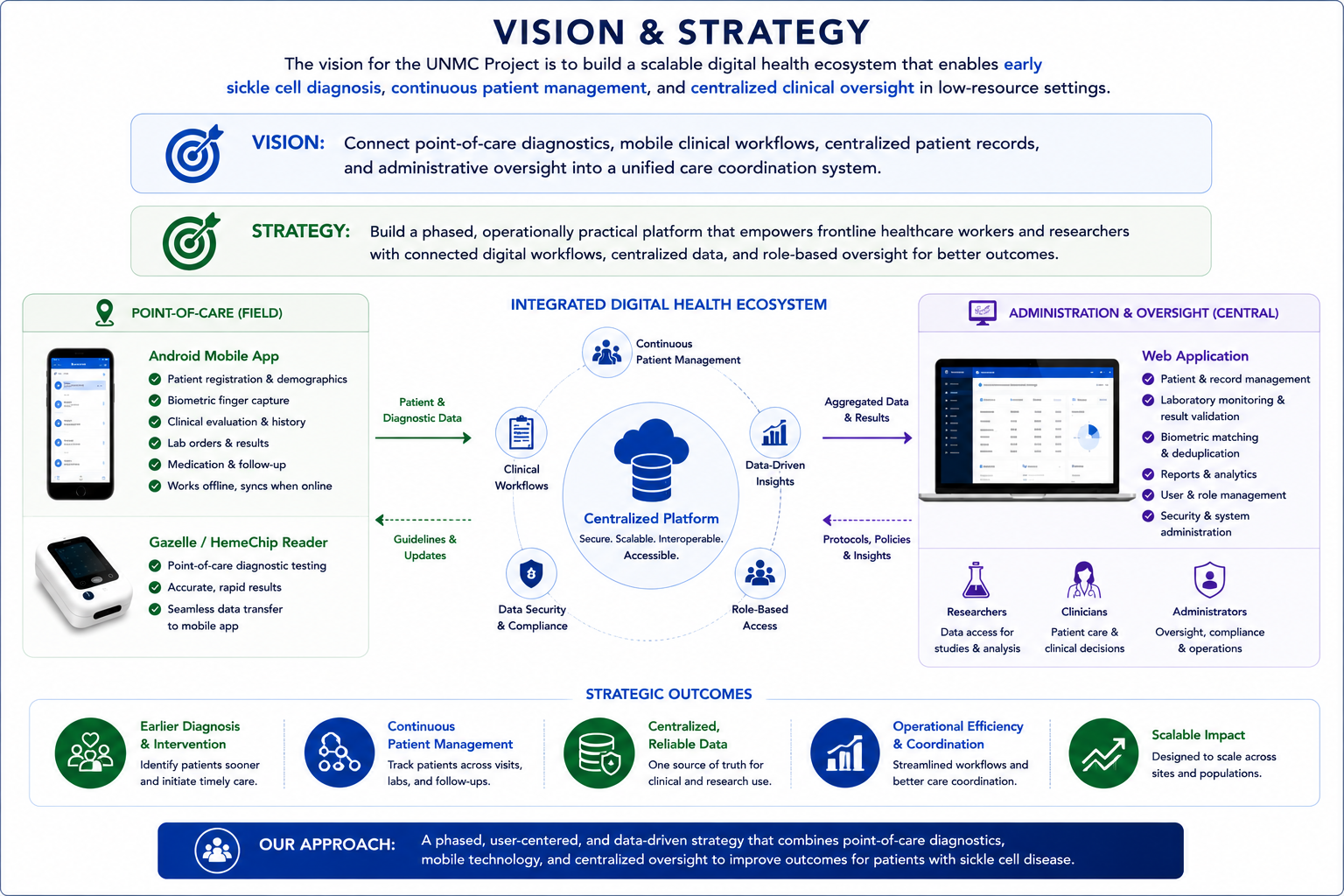
The platform strategy focused on connecting frontline clinical workflows with centralized oversight to create a scalable, data-driven care coordination ecosystem for low-resource healthcare environments.
6. User & Workflow Analysis
A major focus of the UNMC Project was understanding how frontline healthcare workers operated within low-resource clinical environments and translating those realities into practical digital workflows. The platform needed to support a wide range of operational activities including patient registration, guardian management, biometric capture, clinical evaluations, laboratory testing, medication tracking, and follow-up care coordination.
Field workflows were intentionally designed to be structured, guided, and operationally efficient to minimize user error and improve data consistency during active screening activities. The Android application enabled healthcare workers to capture patient demographics, symptoms, medical history, laboratory requests, and diagnostic results directly at the point of care, while supporting offline-first workflows for environments with unreliable connectivity.
At the same time, the web application was designed for centralized administrative and research oversight. Researchers and administrators used the platform to monitor laboratory activities, manage user access, validate clinical data, review aggregated patient records, and perform biometric matching between guardians and patient profiles. This separation between field operations and centralized oversight created a scalable workflow model capable of supporting both clinical care delivery and long-term research coordination.
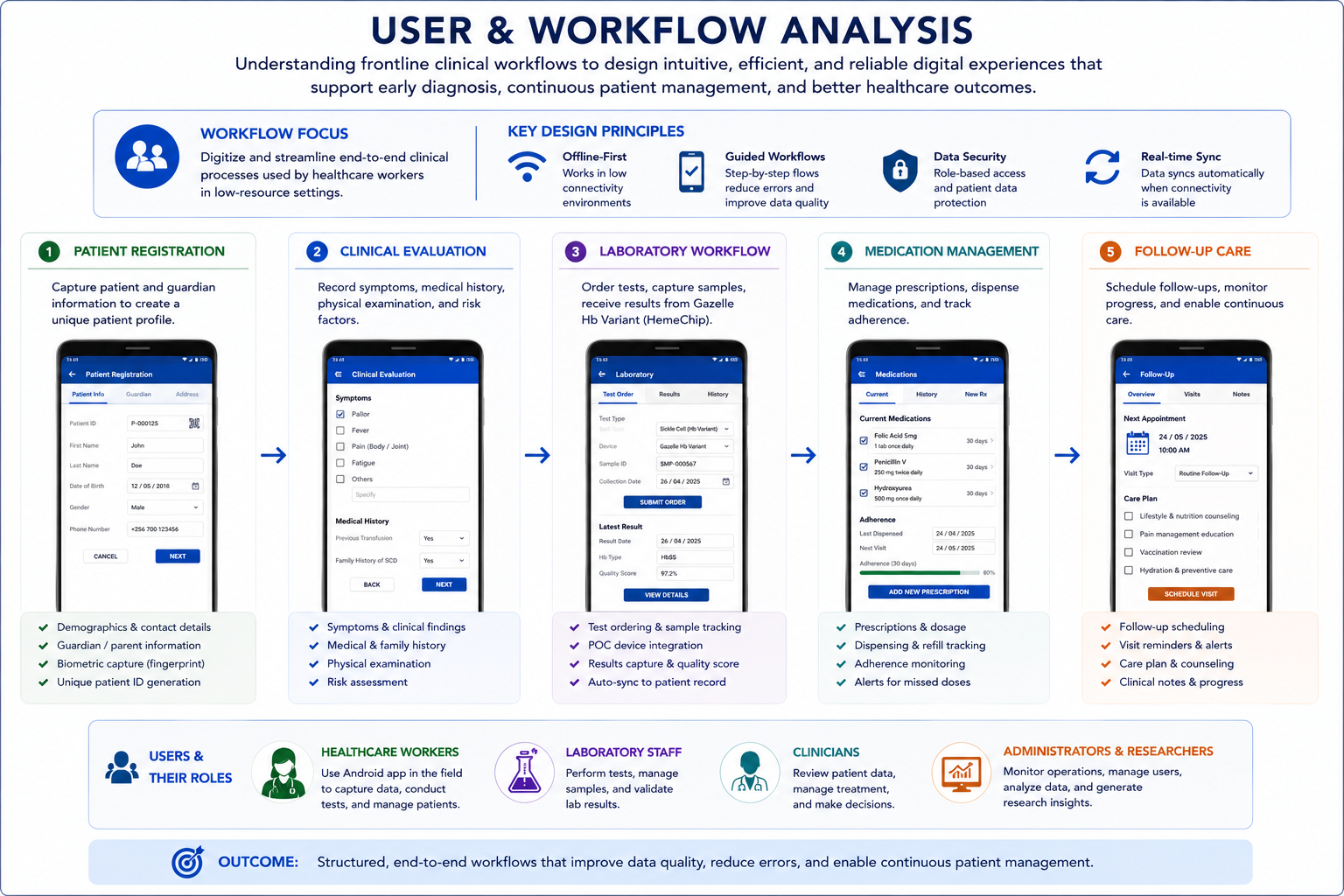
The platform streamlined end-to-end clinical workflows across patient registration, clinical evaluations, laboratory testing, medication management, and follow-up care—enabling healthcare workers to capture reliable patient data and coordinate continuous care in low-resource environments.
7. Solution & System Design
The UNMC Project used a centralized hub-and-spoke architecture to connect point-of-care diagnostics, mobile clinical workflows, and centralized administrative oversight into a unified digital health ecosystem. Clinical and biometric data captured through the Android application, along with diagnostic results from the Gazelle/HemeChip reader, were synchronized into a central electronic database through API-driven integrations and platform connectivity workflows.
The Android application supported frontline healthcare operations including patient registration, guardian management, biometric finger capture, clinical evaluations, laboratory workflows, medication management, and follow-up care. The Gazelle/HemeChip point-of-care diagnostic device integrated with the platform through interoperability services that enabled wireless transmission of hemoglobin electrophoresis results directly into the centralized system.
The web application served as the administrative and research oversight layer, enabling user management, role-based access control, biometric matching, laboratory monitoring, standardized reporting, and review of aggregated patient records. The platform architecture emphasized interoperability, secure data exchange, and scalable integrations between diagnostic hardware, mobile applications, centralized databases, and administrative systems.
The solution was also designed with healthcare interoperability principles in mind, leveraging structured clinical data models, API-based integrations, and platform connectivity patterns aligned with modern healthcare exchange concepts such as HL7 and FHIR-oriented workflows. This architecture created a scalable foundation for continuous patient management, operational visibility, and coordinated clinical decision-making across distributed healthcare environments.
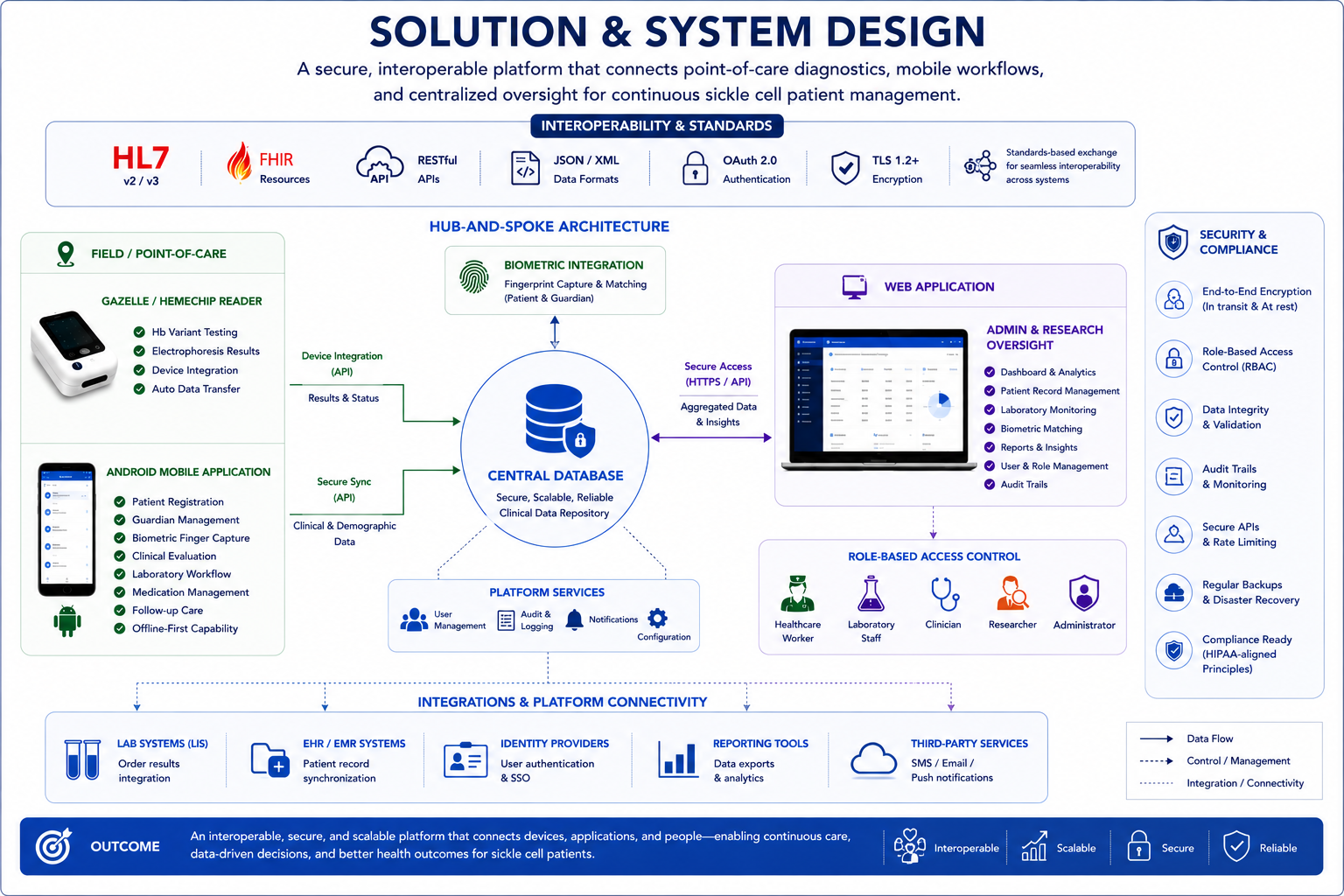
The platform used a centralized hub-and-spoke architecture that integrated point-of-care diagnostics, Android clinical workflows, biometric identity management, APIs, and web-based administrative oversight to enable secure interoperability, continuous patient management, and scalable healthcare operations.
8. Product & Technical Tradeoffs
One of the primary challenges during the UNMC Project was balancing ambitious clinical and operational requirements against the realities of deployment timelines, infrastructure limitations, and evolving hardware dependencies. The platform needed to support complex workflows across diagnostics, biometrics, laboratory management, patient follow-up, and centralized administration while remaining usable within low-resource healthcare environments.
A key product tradeoff involved prioritizing operational simplicity for frontline healthcare workers without compromising the depth of clinical data required by researchers and administrators. The Android application was intentionally designed with guided workflows, simplified navigation, and offline-first capabilities to reduce user friction during active field operations, while the web application handled more advanced administrative, reporting, and oversight responsibilities.
The team also had to balance rapid implementation with interoperability and long-term scalability. Integrating the Gazelle/HemeChip diagnostic device, biometric fingerprint capture, centralized databases, and role-based administrative systems required API-driven integrations and platform connectivity patterns that could support future expansion and evolving healthcare interoperability standards such as HL7 and FHIR-oriented workflows.
Another important tradeoff involved scope prioritization. Advanced automation capabilities, expanded reporting features, and additional workflow enhancements were phased strategically to ensure that core patient registration, laboratory workflows, diagnostic synchronization, and follow-up care processes remained stable and operationally reliable during deployment. This phased delivery approach reduced implementation risk while establishing a scalable technical foundation for future growth.
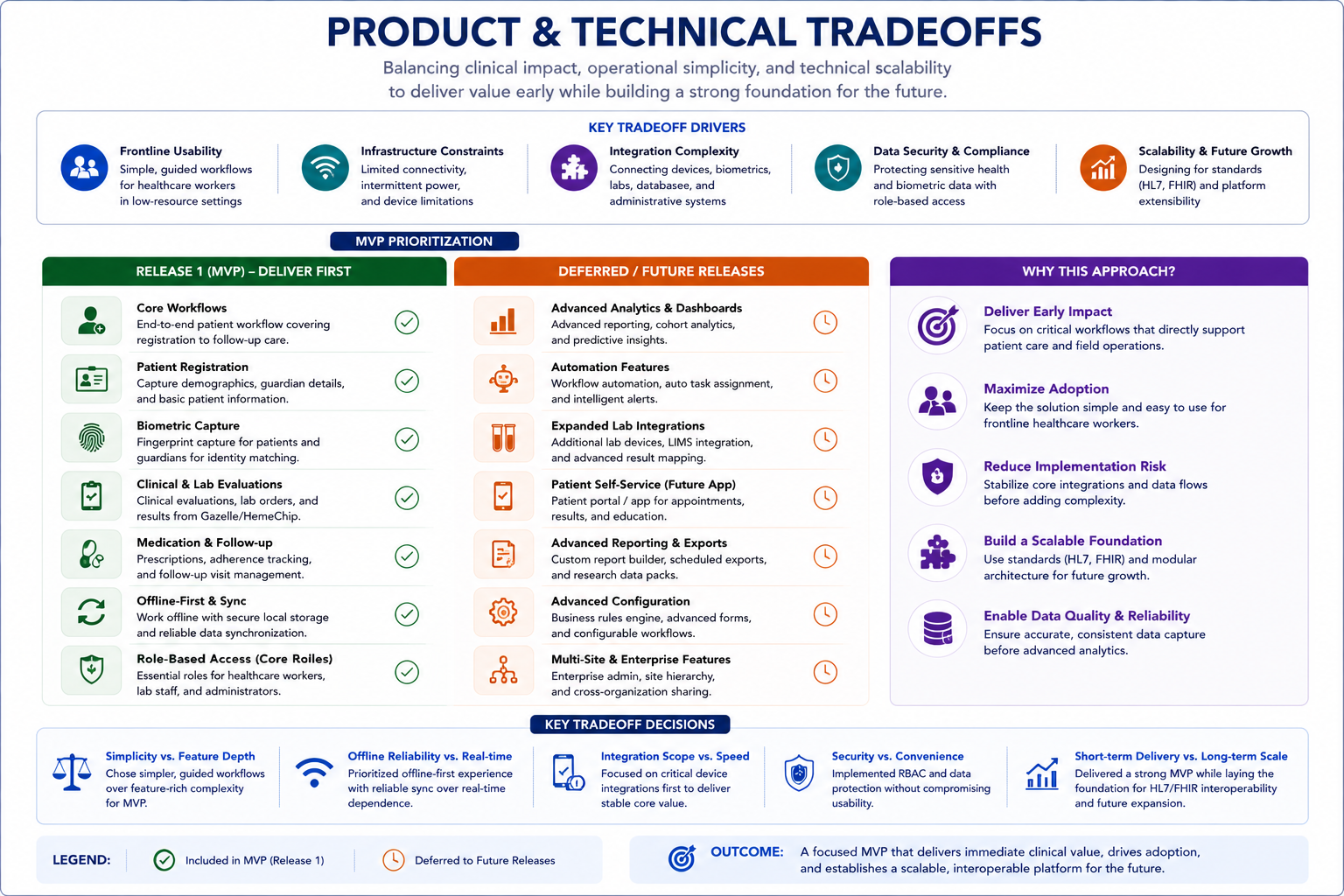
The platform followed a phased MVP strategy that prioritized stable clinical workflows, interoperability, and frontline usability first, while strategically deferring advanced analytics, automation, and enterprise-scale features to future releases.
9. Execution & Cross-Functional Leadership
The UNMC Project required close coordination across multidisciplinary teams including clinicians, researchers, software engineers, laboratory personnel, and operational stakeholders working across distributed environments. As a Business Analyst, I supported cross-functional collaboration by translating clinical and operational requirements into structured workflows, functional specifications, and implementation-ready documentation for the engineering team.
Execution involved continuous alignment between frontline healthcare realities and technical implementation decisions. I worked closely with stakeholders to refine workflows for patient registration, laboratory operations, biometric capture, medication management, and follow-up care while ensuring the platform remained operationally practical for low-resource clinical environments.
The project also required coordination around interoperability and platform connectivity between the Android application, Gazelle/HemeChip diagnostic device, centralized database, and web application. Supporting these integrations required structured requirement management, workflow validation, and ongoing collaboration between technical and non-technical stakeholders to ensure reliable data exchange, operational usability, and system scalability.
Throughout delivery, the team balanced evolving clinical requirements, infrastructure constraints, and deployment timelines through iterative prioritization and phased implementation planning. This collaborative execution model helped establish a scalable digital health platform capable of supporting both frontline clinical workflows and centralized administrative oversight.
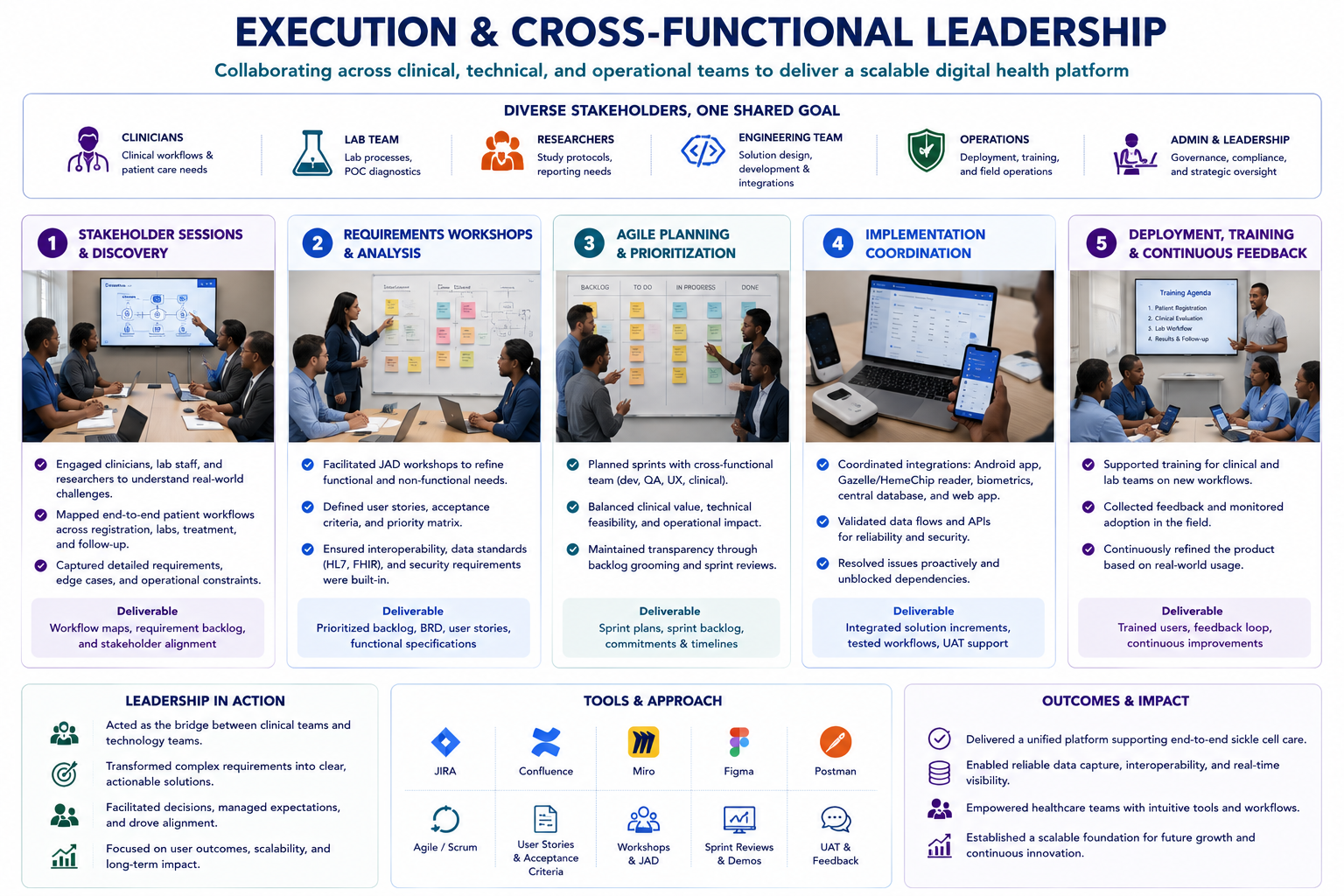
Cross-functional collaboration between clinicians, researchers, engineers, laboratory teams, and operational stakeholders enabled the successful delivery of an interoperable digital health platform aligned with real-world clinical workflows and deployment realities.
10. Metrics & Impact
The UNMC Project established a scalable digital health platform that improved diagnostic workflows, centralized clinical data management, and strengthened coordination between frontline healthcare workers, laboratory teams, researchers, and administrators. By integrating point-of-care diagnostics with connected digital workflows, the platform supported earlier intervention, continuous patient management, and more reliable clinical oversight in low-resource settings.
The Gazelle/HemeChip diagnostic solution achieved 97.2% diagnostic accuracy compared to the clinical gold standard (HPLC), while also demonstrating 100% sensitivity for detecting severe sickle cell variants including HbSS and HbSC. The platform successfully supported data collection, clinical evaluations, and laboratory workflows for hundreds of pediatric patients participating in screening and follow-up programs across Nigeria.
Operationally, the solution improved workflow standardization by digitizing patient registration, biometric identity capture, laboratory evaluations, medication management, and follow-up coordination into a centralized ecosystem accessible through both Android and web applications. The architecture also strengthened interoperability, platform connectivity, and centralized visibility across distributed healthcare environments through API-driven integrations, role-based access controls, and structured clinical data management.
Beyond the technical implementation, the project established a scalable foundation for future healthcare interoperability, research collaboration, and longitudinal patient care coordination across low-resource clinical environments.
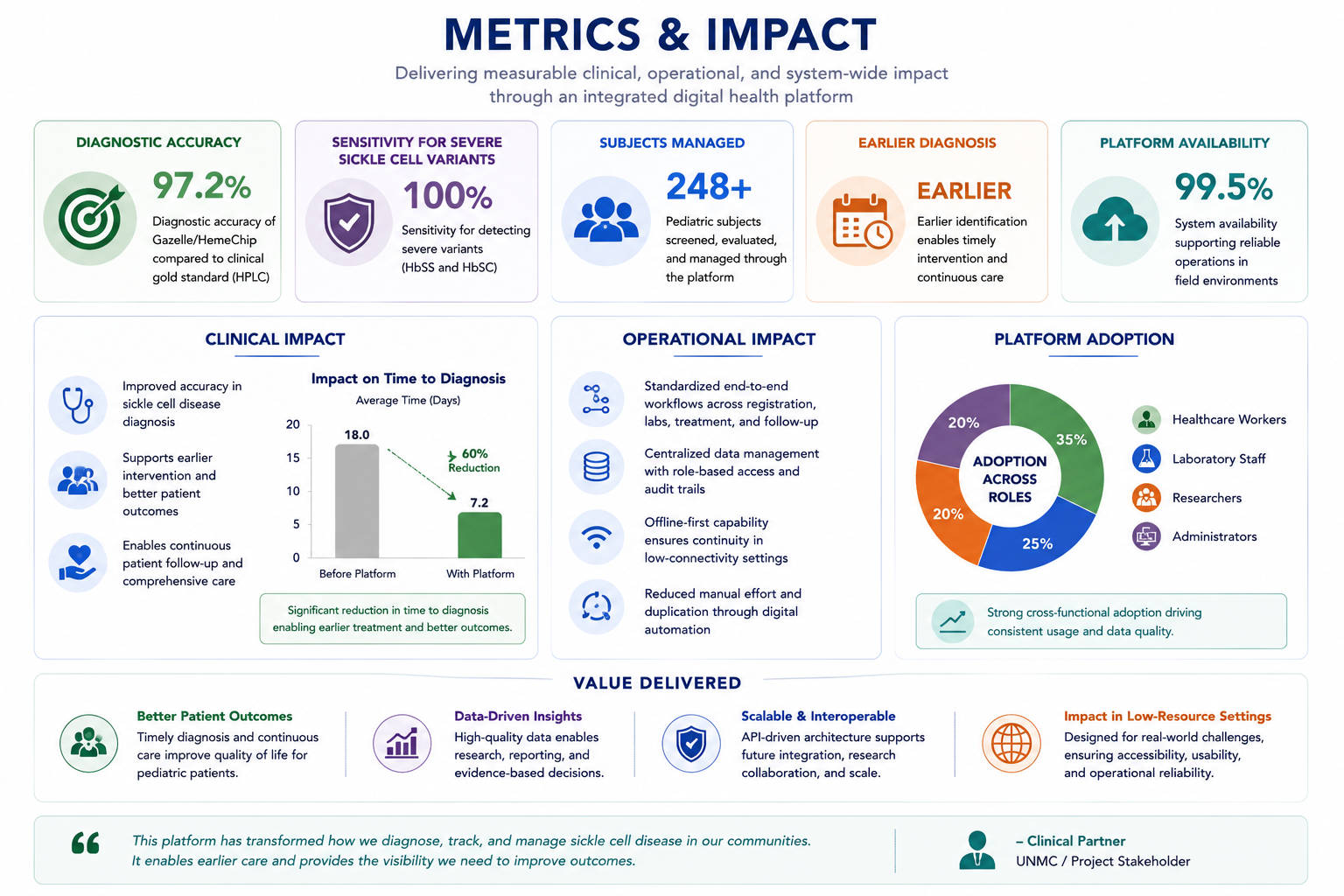
The platform delivered measurable clinical and operational impact by improving diagnostic accuracy, enabling earlier intervention, standardizing healthcare workflows, and strengthening continuous patient management across low-resource clinical environments.
11. Challenges & Lessons Learned
Designing for Low-Resource Clinical Environments
One of the primary challenges was designing a platform capable of supporting complex clinical workflows while remaining simple, reliable, and usable for frontline healthcare workers operating in low-resource environments. Limited connectivity, evolving operational requirements, and varying levels of digital literacy required workflows that were guided, resilient, and operationally practical.
Balancing Technical Complexity with Usability
The platform integrated multiple advanced capabilities including biometric identity management, diagnostic device integrations, centralized reporting, role-based access control, and interoperability workflows. While these features increased architectural complexity, the user experience still needed to remain intuitive for healthcare workers performing patient registration, laboratory workflows, and follow-up care during active field operations.
The Importance of Phased Delivery
The project reinforced the importance of phased implementation and scope prioritization. The team focused first on stabilizing core workflows such as patient registration, clinical evaluations, diagnostic synchronization, medication tracking, and follow-up care. This approach reduced operational risk and established a reliable foundation before expanding into advanced analytics, automation, and enterprise-scale capabilities.
Interoperability as a Long-Term Strategy
Another key lesson was the long-term importance of interoperability and platform connectivity within healthcare systems. Designing around API-driven integrations, structured clinical data models, and healthcare interoperability concepts aligned with HL7 and FHIR-oriented workflows positioned the platform for future scalability, research collaboration, and ecosystem integration.
Technology Alone Is Not Enough
Perhaps the most important lesson was that successful digital health platforms require more than strong technology. Sustainable healthcare transformation depends on aligning clinical realities, operational workflows, user adoption, system scalability, and cross-functional collaboration into a cohesive, user-centered ecosystem capable of supporting continuous patient care.

The project highlighted the importance of adaptability, phased delivery, cross-functional collaboration, and user-centered design when building scalable digital health platforms for complex real-world clinical environments.